Polytrauma
Patients with multiple severe injuries encounter a larger range of complications and a more complex clinical stay than those with severe isolated injuries, e.g. “polytrauma is more difficult to treat than the sum of the isolated injuries”.
The treatment requires knowledge of the complex interplay between several cascade systems that are activated by the injury, the hemorrhage, the ensuing coagulopathy and the activation of inflammation (four vicious cycles). The avoidance of complications through knowledge can save lives.
Therefore, it is necessary that this important subtopic is covered within a society that focuses on the treatment of acute injuries.
The Polytrauma section aims at teaching members of ESTES, visitors of the Annual meeting and readers of scientific Journals the issues of pathophysiology, scientific findings and invovations in treatment of polytrauma patients.
History
An evidence based Definition of Polytrauma was developed by members of the Polytrauma section as follows:
The term ‘polytrauma’ was first used by Tscherne et al. in 1966 for patients that demonstrated a combination of at least 2 ‘severe injuries of the head, chest or abdomen’ or ‘one of them in association with an extremity injury’ In 1975, Border et al. defined the ‘polytrauma’ patient “as any patient with two or more significant injuries”. Oestern et al. then distinguished the entity ‘polytrauma’ as ‘a patient with two or more injuries, one of them being potentially life threatening’ from `isolated, but potentially life threatening injuries`, for which he coined the term ‘barytrauma’.
To address the lack of an evidence based definition, a group of experts met in a series of scientific sessions and meetings. These were held under the auspices of several societies; European Society for Trauma and Emergency Surgery (ESTES), German Trauma Society (DGU), British Trauma Society (BTS), American Association for the Surgery of Trauma (AAST), New Zealand Association for the Surgery of Trauma (ANZAST) The consensus was reached following a number of quality management measures, such as a preparative literature review, multiple in person meetings, and evaluation of data using data from 28.211 polytraumatized patients. The ensuing parameters consisted of five pathologic conditions and ancillary parameters to describe a multiply injured patient.
The definition of polytrauma revisited: An international consensus process and proposal of the new ‘Berlin definition’ Pape HC, Lefering R, Butcher N, Peitzman A, Leenen L, Marzi I, Lichte P, Josten C, Bouillon B, Schmucker U, Stahel P, Giannoudis P, Balogh Z. J Trauma Acute Care Surg. 2014 Nov;77(5):780-786.
Section Board


Active Polytrauma Section Members
Zsolt Balogh, Andrej Čretnik, Luca Fattori, Sascha Halvachizadeh, Falco Hietbrink, Frank Hildebrand, Klemens Horst, Diego Mariani, Ingo Marzi, Thomas Mendel, Hans Christoph Pape, Roman Pfeifer; Inger B Schipper, Hans-Peter Simmen, Philipp Störmann, Klaus Wendt
February 2024 ==> 347 Participants
Section Meeting Minutes
Minutes Consensus Meeting 2019 09 12
Minutes Consensus Meeting 2019 05 05
Section Meeting Agenda 2019
Minutes Steering Board Meeting 2019 01 10
Agenda Steering Board Meeting 2018 09 20
Minutes Steering Board Meeting 2018 09 20
Section Meeting Minutes 2018
Section Meeting Minutes Estoril 2024
Section Meeting Minutes Aachen 2025
Projects
Publications
Articles/ Position Papers
Indications and interventions of damage control orthopedic surgeries
an expert opinion survey 2020
The definition of polytrauma revisited
An international consensusprocess and proposal of the new ‘Berlin definition’ 2014
Documentation of Blunt Trauma in Europe 2000
Standards of fracture care in polytrauma: results of a Europe-wide survey by the ESTES polytrauma section – PubMed (nih.gov)

Early major fracture care in polytrauma-priorities in the context of concomitant injuries: A Delphi consensus process and systematic review – PubMed (nih.gov)
Free Polytrauma APP
The APP has been developed in 2016 and is available for Android and IOS. It is free and demonstrates all relevant scoring systems to be used in the emergency room and thereafter. It
The APP has been developed in 2016 and is available for Android and IOS. It is free and demonstrates all relevant scoring systems to be used in the emergency room and thereafter. It
Courses
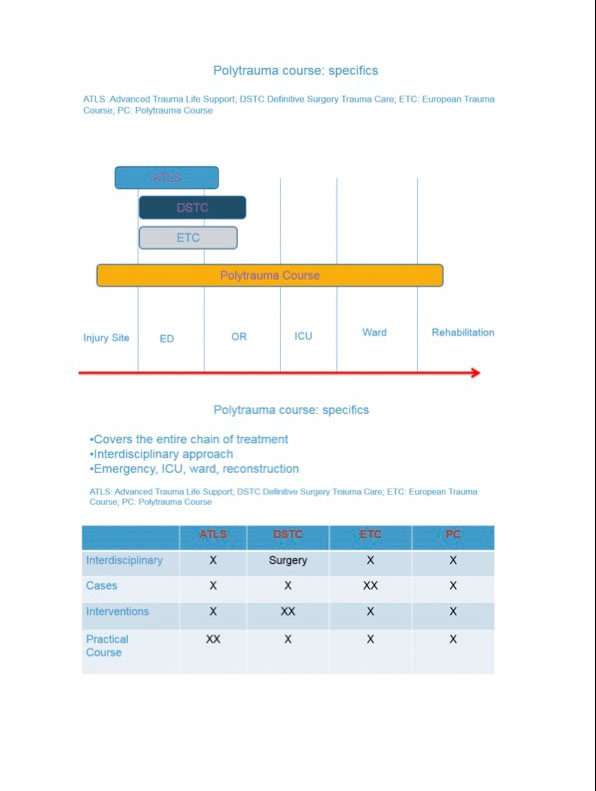
Polytrauma Course
The hallmark of the Polytrauma section is represented by the Polytrauma course, which is structured as a 2 day course. www-polytraumacourse.com It is guided by a Polytrauma course steering board